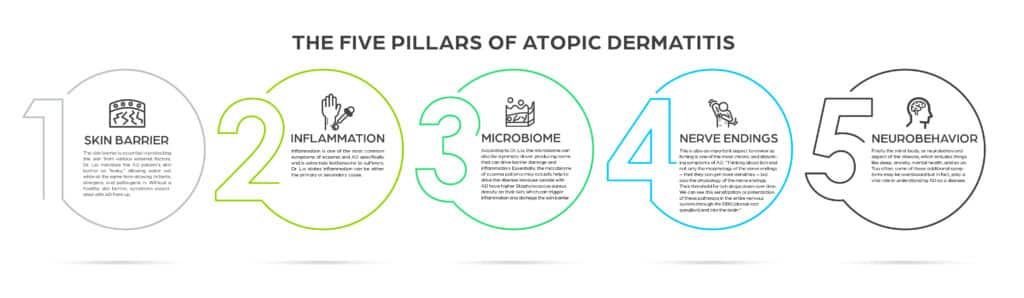
The skin barrier is essential in protecting the skin from various external factors. Dr. Lio mentions the AD patient’s skin barrier as “leaky”, allowing water out while at the same time allowing irritants, allergens, and pathogens in. Without a healthy skin barrier, symptoms associated with AD flare up.
Inflammation is one of the most common symptoms of eczema and AD specifically and is extremely bothersome to sufferers. Dr. Lio states inflammation can be either the primary or secondary cause.
![]()
According to Dr. Lio, the microbiome can also be a primary driver, producing toxins that can drive barrier damage and inflammation. Essentially, the microbiome of eczema patients may actually help to drive the disease because people with AD have higher Staphylococcus aureus density on their skin, which can trigger inflammation and damage the skin barrier.
This is also an important aspect to review as itching is one of the most chronic and disturbing symptoms of AD.
![]()
Finally the mind-body, or neurobehavioral aspect of the disease, which includes things like sleep, anxiety, mental health, and so on. Too often, some of these additional symptoms may be overlooked but in fact, play a vital role in understanding AD as a disease.